
The Metabolic Roots of Autoimmune and Thyroid Disease
She had been managing her Hashimoto's for four years. On levothyroxine, TSH in range, a good relationship with her endocrinologist. She was not satisfied. In four years of clinical management, nobody had tested her fasting insulin. Her HOMA-IR was 6.3. She had significant insulin resistance — almost certainly for most of the time she'd had Hashimoto's — and it had never been named, never connected to the fatigue, the weight, the brain fog, or the steadily rising antibody levels.
This is the episode that sits at the intersection of my deepest clinical specialism and April's metabolic theme. Last week I laid out the insulin resistance picture — what it is, why standard testing misses it, what it does downstream. This week I want to take that framework and apply it directly to autoimmune and thyroid disease. Because the central clinical argument I want to make is this:
Autoimmune and thyroid conditions are not purely immunological problems. They have a metabolic substrate. And most patients receiving specialist care are being managed for the immune or hormonal manifestation of their condition without anyone assessing or addressing the metabolic environment actively sustaining it.
The Inflammatory Bridge: How Insulin Resistance Drives Immune Dysregulation
The mechanism begins with visceral adipose tissue — the fat deposited around the abdominal organs that accumulates as insulin resistance develops. Visceral fat is not metabolically inert. It is an active inflammatory endocrine organ. And its output directly disrupts immune regulation.
Visceral adipocytes overproduce pro-inflammatory cytokines: TNF-alpha, interleukin-6, interleukin-1 beta. These cytokines activate NF-kB — the master transcription factor for inflammatory gene expression — in immune cells simultaneously. IL-6 in particular drives the differentiation of T cells towards the pro-inflammatory Th17 phenotype rather than the regulatory Treg phenotype.
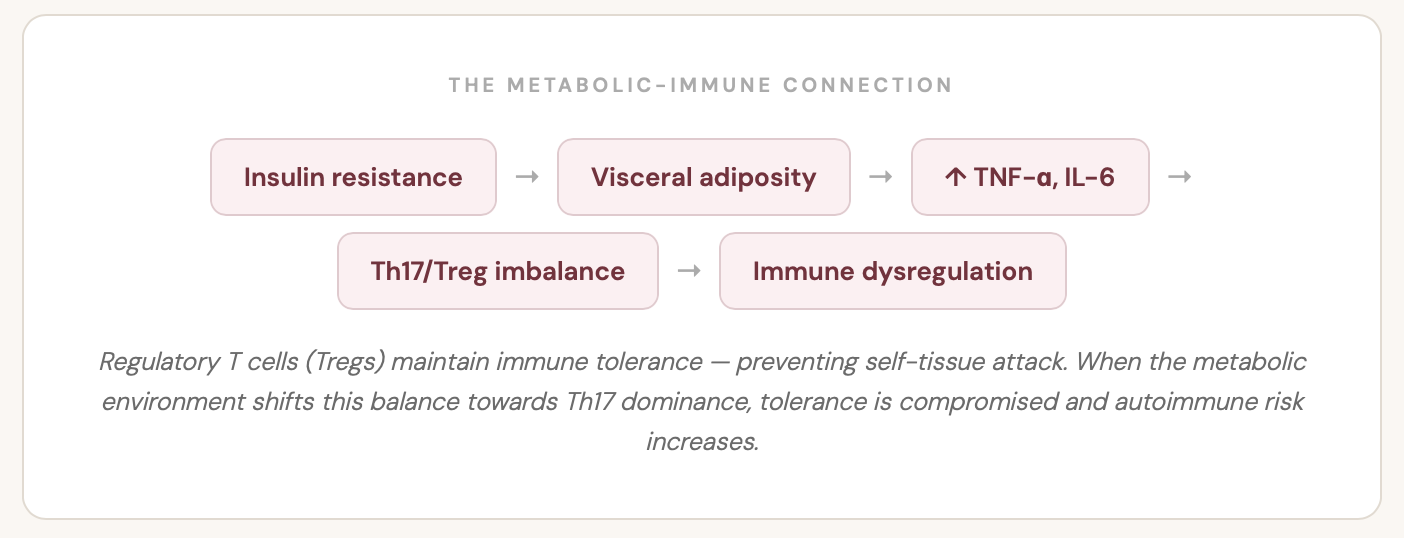
The Th17/Treg balance is central to autoimmune disease. Regulatory T cells are the immune system's governors — their job is to prevent the immune system from attacking the body's own tissue. In the chronic low-grade inflammatory environment produced by visceral adiposity and insulin resistance, that balance shifts. Tolerance is compromised. Established autoimmune disease worsens.
“Managing the autoimmune condition without addressing the metabolic environment is treating the fire without addressing the accelerant.”
There is a second mechanism through the adipokines — specifically leptin and adiponectin. Leptin rises with increasing adiposity and is pro-inflammatory in its immune effects, promoting aggressive immune responses and suppressing Treg function. Adiponectin — anti-inflammatory, Treg-supporting — falls as visceral fat accumulates. In insulin resistance, you get elevated leptin and reduced adiponectin simultaneously, removing one of the body's primary endogenous anti-inflammatory signals at precisely the moment when the inflammatory load is rising.
The Thyroid-Metabolic Axis: Why "Normal TSH" Isn't the Whole Story
The relationship between insulin resistance and thyroid function is one of the most clinically significant connections in my practice, and one of the most consistently overlooked. Let me explain the mechanism precisely.
Thyroid hormone is produced primarily as T4 — thyroxine — the inactive prohormone. To become biologically active, T4 must be converted to T3 (triiodothyronine) — the form that binds to thyroid hormone receptors in every cell and drives metabolic rate, energy production, and cellular function. This conversion is carried out by deiodinase enzymes in the liver, kidneys, gut, and peripheral tissues.
And it is exquisitely sensitive to the metabolic environment. Insulin resistance, chronic inflammation, elevated cortisol, and nutrient deficiencies — particularly selenium and zinc — all impair deiodinase activity and reduce T4-to-T3 conversion efficiency.
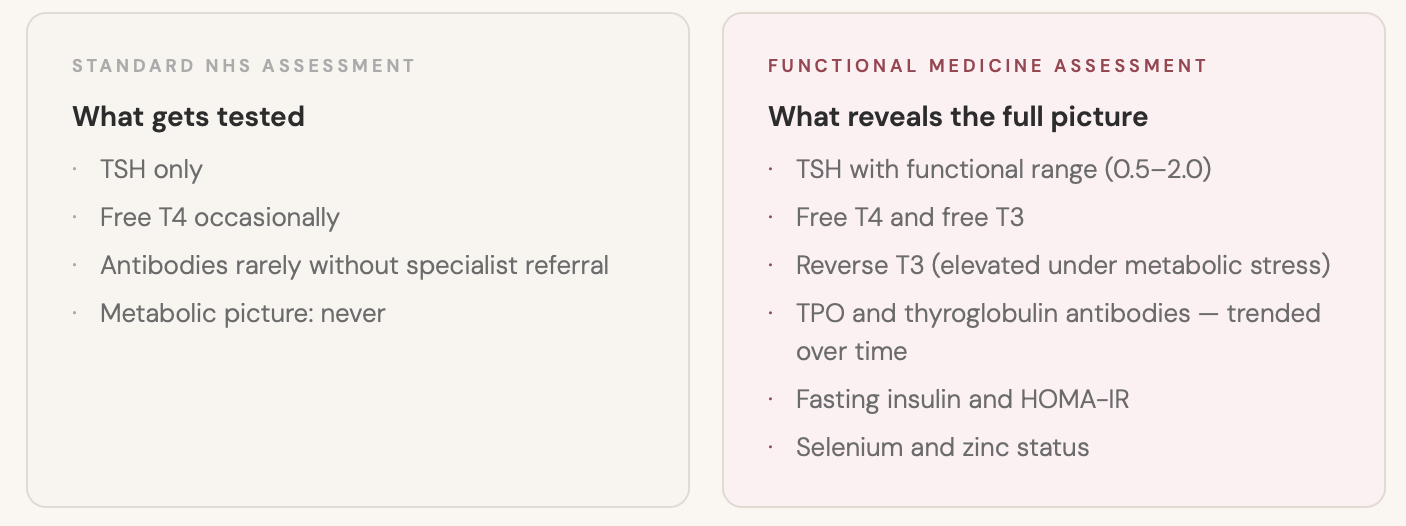
This is the mechanism behind one of the most common patterns I see: normal TSH, normal T4, low or low-normal free T3. The thyroid is producing hormone. The hormone isn't being efficiently converted. The patient is symptomatic. And because the standard panel only checks TSH, the conversion problem — driven by metabolic inflammation — is completely invisible.
HASHIMOTO'S AND ANTIBODY TITRES
TPO antibodies are not simply a diagnostic marker. They are a measure of ongoing autoimmune activity against thyroid tissue. High antibodies mean the immune system is actively attacking the thyroid. Reducing antibody titres means reducing the rate of destruction — preserving function and, in some cases, achieving genuine remission.
The interventions that move antibody titres are primarily metabolic and nutritional: selenium supplementation at 200 mcg (which showed significant TPO antibody reductions across nine RCTs in a 2016 meta-analysis), vitamin D correction, gut repair, and critically — addressing insulin resistance. The chronic Th17-dominant immune environment produced by insulin resistance is one of the most significant drivers of continued antibody production. You cannot meaningfully reduce Hashimoto's antibody titres in a patient with a HOMA-IR of 5.0 without addressing the metabolic environment. The immune system will not allow it.
The Broader Autoimmune Spectrum
The metabolic-autoimmune connection is not specific to Hashimoto's. It runs across the full autoimmune spectrum, driven by the same Th17/Treg imbalance and adipokine dysregulation playing out in different target tissues.
Rheumatoid Arthritis
Insulin resistance is both more prevalent in RA patients than matched controls and positively associated with disease activity. Anti-TNF biologics improve insulin sensitivity as a secondary effect — a mechanistic demonstration that inflammatory activity and metabolic function are directly linked. Improving insulin sensitivity through dietary intervention reduces circulating TNF-alpha and IL-6, reducing RA disease activity independently of medication.
Lupus (SLE)
Lupus patients carry cardiovascular risk up to 50 times higher than age-matched controls. Insulin resistance is significantly more prevalent and associated with higher disease activity. Hydroxychloroquine — a primary lupus medication — has a well-documented insulin-sensitising effectconsidered one mechanism of its beneficial disease-modifying action. This is pharmacological evidence that metabolic improvement is a legitimate therapeutic target in lupus.
Psoriasis
Metabolic syndrome is significantly more prevalent in psoriasis than in the general population. The skin inflammation and systemic metabolic dysfunction are driven by the same mediators: TNF-alpha, IL-17, IL-23. In clinical practice, psoriasis patients who address their insulin resistance consistently achieve better outcomes — fewer flares, better treatment response — than dermatological management alone produces.
What the Joined-Up Assessment Looks Like in Practice
When a patient comes to me with a thyroid or autoimmune condition, the assessment covers four layers simultaneously. This is what separates a functional medicine evaluation from a conventional single-system assessment — and it is what reveals the picture that four years of specialist care had missed for the patient in today's episode.
LAYER 1
Metabolic
Fasting insulin and HOMA-IR. Fasting glucose and HbA1c. Triglyceride-to-HDL ratio. Uric acid — an independent marker of insulin resistance and fructose load. Liver enzymes (ALT and GGT) as markers of hepatic insulin resistance. ApoB or advanced lipid assessment — because in insulin resistance, standard LDL can be normal while the particle composition is pro-atherogenic.
LAYER 2
Thyroid Axis
TSH with functional range interpretation — targeting 0.5–2.0 rather than accepting 3.8 as "within range." Free T4. Free T3. Reverse T3 — elevated under metabolic stress and frequently explaining ongoing symptoms that normal T4 and TSH cannot. TPO and thyroglobulin antibodies trended over time as measures of disease activity, not merely diagnostic markers.
LAYER 3
Inflammatory
High-sensitivity CRP for systemic inflammatory load. Homocysteine — relevant both as a cardiovascular risk marker and as an indicator of B vitamin status and methylation. Vitamin D (25-OH) — below 75 nmol/L is nearly universal in autoimmune patients and its correction is one of the most impactful single interventions available. Ferritin, zinc, and selenium.
LAYER 4
Gut
Comprehensive stool analysis for microbiome composition and gut inflammation markers — calprotectin and lactoferrin reflect intestinal immune activation. Intestinal permeability markers where clinically indicated. Dietary history to identify the gut-specific drivers of inflammatory load. Approximately 20% of thyroid hormone conversion occurs in the gut — gut health is directly relevant to thyroid function.
THE CLINICAL OUTCOME OF JOINING THE PICTURE UP
The patient in today's episode — four years of Hashimoto's management, levothyroxine stable, still profoundly unwell — began a metabolic protocol alongside her existing treatment. Dietary change for insulin sensitivity. Targeted nutritional support including selenium, vitamin D, and gut repair. Stress physiology addressed explicitly.
Within eight weeks her free T3 improved. Her reverse T3 fell. Her TPO antibodies — persistently elevated since diagnosis, never expected to move — began, for the first time, to decline. Her energy changed in a way that four years of levothyroxine management alone had not achieved.
Her conventional care was good. What was missing was the metabolic layer. Not instead of her specialist care — alongside it. That is what the joined-up picture looks like when it is actually joined up.
If you have a thyroid or autoimmune condition
The 7 Day Reset provides the dietary and nutritional foundation for the metabolic work — blood sugar stabilisation, inflammatory load reduction, insulin sensitivity support.