
Insulin Resistance: The Hidden Driver Behind Your Fatigue, Brain Fog and Weight
She was doing everything right. Clean diet. Regular exercise. Reasonable sleep. Her blood tests came back normal — twice. And she still crashed every afternoon, couldn't shift the weight, and woke up tired after eight hours. Her fasting glucose was 5.1. Normal. Her fasting insulin was 22. That number changed everything.
April is metabolic health month. And I want to start at what I consider the beginning of the metabolic story — not because it's trendy, but because in my clinical experience, insulin resistance is the single most common driver of the symptom cluster that brings people to me: the fatigue, the brain fog, the weight that won't shift, the energy crashes, the poor sleep, the low mood, the sense that the body is working against you.
These are not separate problems requiring separate solutions. In many cases, they are one metabolic problem with multiple expressions. And that problem has been present — quietly, measurably, consequentially — for years before any standard test flags it.
What Insulin Resistance Actually Is
Insulin is the hormone produced by the pancreas that acts as a key — opening the door on your cells so that glucose from the bloodstream can enter and be used for energy. In a healthy system: you eat, blood sugar rises, insulin rises in response, glucose enters cells, blood sugar returns to baseline, insulin falls. A clean, self-regulating cycle.
Insulin resistance is what happens when that key stops fitting the lock properly. The cells — primarily muscle, liver and fat cells — become less responsive to insulin's signal. Glucose cannot enter efficiently. Blood sugar starts to rise. The pancreas responds by producing more insulin to compensate — essentially shouting louder to get the same response.
And here is the critical piece: for a while, this compensation works. Blood sugar stays controlled. From a standard fasting glucose test, everything looks normal. But behind that normal glucose reading, insulin is running at two, three, sometimes four times the level it should be — working overtime to maintain what appears to be normal function.
“The absence of a raised fasting glucose does not mean the absence of a metabolic problem. Insulin resistance can be present — and consequential — for a decade before glucose rises.”
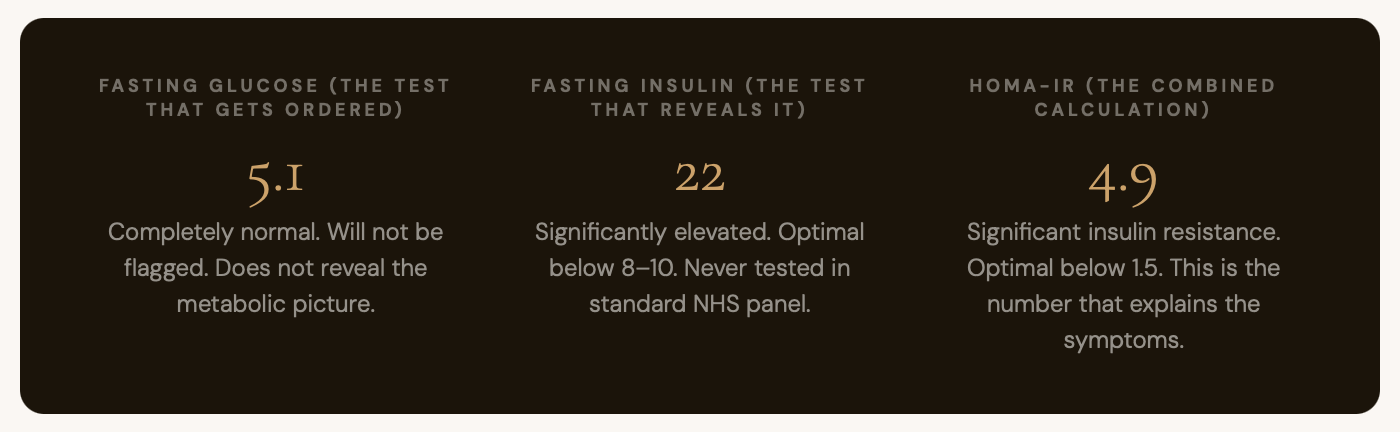
This was the patient I described at the start. Normal fasting glucose. Significantly elevated insulin. A HOMA-IR — the calculation that combines both to give a measure of insulin sensitivity — of 4.9. She had significant insulin resistance. Almost certainly for several years. And it explained, at the mechanistic level, almost everything she had been experiencing.
What Drives It: The Five Main Causes
The primary driver is chronic hyperinsulinaemia — chronically elevated insulin itself. And what drives that? A diet high in refined carbohydrates and sugar, delivered repeatedly across years. But diet is not the only driver, and this matters clinically — because I see insulin resistance in patients with reasonably good diets who are confused about why their metabolic markers are off.
1. Refined carbohydrate and sugar load
Every blood sugar spike drives an insulin spike. Repeated across years, cells downregulate their insulin receptors — desensitised by the constant signal. Fructose specifically, as found in processed foods and high-fructose corn syrup, drives hepatic insulin resistance directly through the liver.
2. Chronic sleep deprivation
A landmark study restricting healthy adults to 4 hours of sleep for just 6 nights reduced insulin sensitivity by 30% — comparable in metabolic effect to gaining 10–15kg of body weight. Even habitual short sleep of 6 hours is associated with significantly elevated HOMA-IR. Sleep is a metabolic intervention, not a lifestyle preference.
3. Chronic stress and cortisol
Cortisol and insulin are metabolic antagonists. Cortisol raises blood glucose; insulin lowers it. In a state of chronic HPA activation — the sustained stress load that characterises so many people's lives — cortisol is chronically driving blood sugar up, chronically requiring insulin to compensate. The stress-metabolic axis is one story, not two.
4. Physical inactivity and low muscle mass
Skeletal muscle is the primary site of insulin-mediated glucose uptake. Low muscle mass or sedentary behaviour significantly reduces insulin sensitivity — which is why resistance training is one of the most powerful metabolic interventions available, not a secondary nice-to-have.
5. Visceral adipose tissue
Fat stored around the abdominal organs produces its own inflammatory cytokines that directly impair insulin signalling at the cellular level. Visceral fat is not metabolically inert — it is an active, inflammatory endocrine organ. Its accumulation both results from and drives insulin resistance in a self-reinforcing cycle.
The Downstream Cascade: What Insulin Resistance Does to Your Whole System
This is where the clinical picture expands dramatically — because insulin resistance is not simply a blood sugar problem. As it progresses, chronically elevated insulin and the inflammatory environment it creates affect virtually every system in the body.
Brain and cognition: The brain is profoundly insulin-sensitive. Insulin resistance impairs neuronal glucose uptake — the brain's fuel delivery system. You feel this as brain fog, cognitive slowness, poor concentration, and memory issues. The connection between insulin resistance and neurodegenerative disease is now sufficiently established that some researchers refer to Alzheimer's as "type 3 diabetes."
Energy and mitochondria: Chronically elevated insulin suppresses fat oxidation — it is powerfully anti-lipolytic. The body cannot efficiently burn its own fat stores for fuel. You're stuck running on glucose, which crashes every few hours. The afternoon energy crash is not a willpower problem. It is a fuel metabolism problem.
Sex hormones: Elevated insulin directly stimulates the ovaries to produce excess androgens and disrupts sex hormone binding globulin, lowering free oestrogen and testosterone. This is the primary mechanism behind PCOS, and it contributes to the hormonal disruption of perimenopause.
Sleep architecture: Insulin resistance disrupts nocturnal glucose dynamics, increases cortisol nocturnal peaks, and impairs the deep sleep stages where metabolic restoration occurs. You can sleep eight hours and wake exhausted because the architecture of the sleep — not just the duration — is compromised.
Mood and mental health: Dopamine and serotonin pathways are sensitive to the same insulin signalling disruptions that affect energy metabolism. Low mood, anxiety, and emotional dysregulation are common features of unaddressed insulin resistance — and are rarely connected to it clinically.
Immune function and inflammation: Visceral adiposity drives a chronic pro-inflammatory cytokine environment — elevated TNF-alpha, IL-6, IL-1β — that dysregulates immune function in the same way stress does. The metabolic-immune axis is directly relevant to anyone with autoimmune or thyroid disease — which is exactly what we'll cover next week.
Why Women in Their 30s and 40s Are Disproportionately Affected
This is one of the most clinically underappreciated aspects of the insulin resistance story. Three factors converge in this demographic in a way that is rarely joined up in conventional care.
The oestrogen piece: Oestrogen is insulin-sensitising. It promotes glucose uptake in muscle tissue and supports healthy body composition. As oestrogen begins to fluctuate and decline in perimenopause — which can begin as early as the mid-thirties — that protective effect diminishes. The same dietary patterns that were metabolically tolerated at 32 may begin to drive metabolic dysfunction at 38 or 42. The body has not failed. The hormonal environment has changed.
The cortisol piece: Managing careers, families, relationships, and often their own health without adequate support — the chronic HPA activation this creates is a direct metabolic driver, as described above. Stress is not a separate story from metabolic health. They share the same hormonal infrastructure.
The diagnostic gap: Fatigue is attributed to a busy life. Brain fog is attributed to perimenopause or stress. Weight gain is attributed to ageing or dietary failure. Low mood is attributed to anxiety or depression. None of these are wrong as observations — they are all genuine features of this life stage. But they are also metabolic signals, and the metabolic layer is consistently missed because it is not looked for.
THE THREE NUMBERS WORTH KNOWING
If you take one practical thing from this post: at your next blood test, ask specifically for fasting insulin alongside fasting glucose. Some GPs will agree; some won't. If you have private testing access, this is the highest-yield single addition to a standard panel.
Fasting insulin optimal: below 8–10 mIU/L. HOMA-IR (calculated from insulin × glucose ÷ 22.5) optimal: below 1.5. A result of 3, 4, or 5 is significant insulin resistance — regardless of whether fasting glucose is flagged as normal.
The triglyceride-to-HDL ratio on a standard lipid panel is a useful proxy: a ratio above 2.0 (using mmol/L) is strongly associated with insulin resistance and small dense LDL particle pattern — the atherogenic profile that standard LDL measurement misses entirely.
What Actually Moves the Metabolic Picture
Insulin resistance is one of the most reversible metabolic conditions managed in functional medicine. That is a direct statement, not a qualified one. With the right approach, insulin sensitivity can be meaningfully and measurably improved within weeks. Here are the main levers.
LEVER 1 — MOST IMPACTFUL
Reduce glycaemic load — not calories, carbohydrate quality
Replacing refined carbohydrates and added sugars with whole food carbohydrates paired with fibre, protein and fat directly reduces the insulin demand on the pancreas. A systematic review of low-carbohydrate diets found significantly greater improvements in fasting insulin and HOMA-IR than low-fat diets at 6 and 12 months. Prioritise non-starchy vegetables, legumes, berries over high-sugar fruits, and eliminate liquid calories from sugar — which delivers fructose without the fibre that would slow absorption.
LEVER 2
Protein at every meal — minimum 25–30g
Protein has a minimal insulin response relative to carbohydrate and stimulates glucagon — counteracting insulin and promoting metabolic balance. Adequate protein at each meal stabilises postprandial glucose, supports satiety, and is essential for maintaining the muscle mass that is the primary site of insulin-mediated glucose uptake. You cannot meaningfully improve insulin sensitivity without preserving or building muscle.
LEVER 3 — HIGHEST YIELD PER MINUTE
Post-meal walking — 10 minutes changes the glucose picture
Muscle contraction drives glucose uptake through an insulin-independent pathway (GLUT4 transporter translocation) — meaning movement improves glucose clearance even when insulin signalling is impaired. A 2022 systematic review found that a 10-minute walk after eating significantly reduced postprandial glucose and insulin compared to sitting. No equipment. No gym membership. This is one of the highest-yield, lowest-cost metabolic interventions available.
LEVER 4
Resistance training — build the glucose disposal system
Resistance training builds muscle mass — increasing the total capacity for glucose disposal — and the metabolic effect of a single session lasts 24–48 hours. This is not about aesthetics. It is about building the primary tissue responsible for clearing glucose from the bloodstream. For women in their 30s and 40s navigating the oestrogen decline that reduces natural insulin sensitivity, resistance training is close to non-negotiable.
LEVER 5 — NUTRITIONAL SUPPORT
Magnesium, berberine, inositol — direct insulin sensitivity support
Magnesium is a cofactor in insulin receptor activation — deficiency is associated with insulin resistance across multiple studies. Berberine has been shown in meta-analyses to reduce fasting insulin and HOMA-IR comparably to metformin through AMPK activation — the same pathway activated by exercise. Inositol (myo and D-chiro forms) has strong RCT evidence for restoring insulin signalling in PCOS specifically. These are additions to dietary and lifestyle change, not replacements for it.
Begin the metabolic work
The 7 Day Reset is specifically designed to begin blood sugar stabilisation and reduce the dietary inflammatory load — the foundation of the metabolic framework we've covered here.