
The 'Normal' Results Trap: What Functional Medicine Looks For That Your GP Doesn't Test
You've had the blood tests. Everything came back normal. Your GP said there's nothing to find. And you walked out of that appointment still exhausted, still foggy, still feeling like your body is fighting something — with the added layer of being told, implicitly, that it might all be in your head. Here's what normal actually means. And what it doesn't.
I want to start with a word. Normal.
In medicine, "normal" is a statistical term. It means your result falls within the range seen in most people who have been tested with that particular assay. It does not mean optimal. It does not mean that your body is functioning well. It does not mean that your result is not a credible explanation for how you feel.
Normal is derived from population averages. And population averages include a lot of people who are not well. In a population where metabolic dysfunction is widespread, where chronic stress is the norm, where nutritional depletion is common — the average is not a particularly ambitious health target.
“‘Normal’ in conventional medicine and ‘optimal’ in functional medicine are two completely different things — and the gap between them is where most of my patients have been living for years.”
This isn't a criticism of GPs. They work within a system with limited time and specific testing protocols designed to rule out acute disease and serious pathology. That's important work. But it is not the same as asking whether your physiology is functioning optimally. And when you leave a GP appointment with "normal" results still feeling awful, the problem is often not that there is nothing to find. The problem is that the tests ordered are not designed to find it.
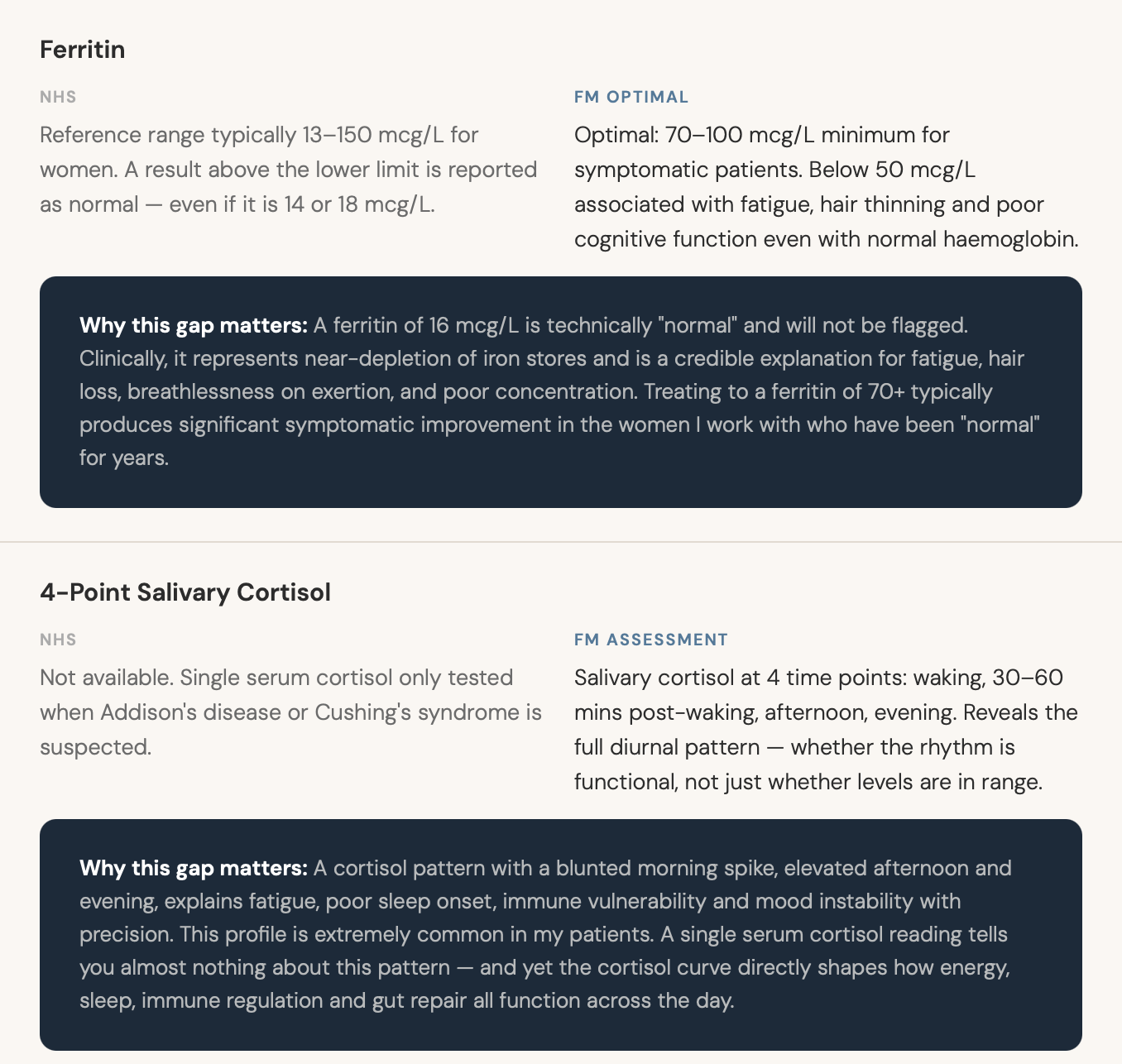
Five Key Markers — and the Gap That Matters
In this week's episode, I walk through five specific markers that consistently reveal the picture behind "normal" — and the gap between what NHS standard ranges report and what functional medicine considers optimal.

What to Do With This Information
I want to be practical here, because information without a clear next step is frustrating rather than helpful.
At your next GP appointment:Ask specifically for fasting insulin (not just fasting glucose), ferritin (and ask where in the range your result falls), and hs-CRP. Some GPs will agree. Some won't. But asking the question — "where in the range is my ferritin, and what would optimal look like?" — starts a different conversation.
If you're paying for private testing:A full thyroid panel (TSH, free T4, free T3, reverse T3, antibodies) and a salivary cortisol profile are the two most revealing tests I use in initial functional medicine assessments for the pattern of symptoms I see most commonly.
Ask the right question:Not "is it normal?" but "where in the range is it, and is that truly optimal for how I feel?" That reframe changes what you're looking for — and what you ask your practitioner to explain.
THE QUESTION NOBODY ASKED
One of the most striking conversations I have regularly in clinic is with patients who have been on thyroid medication for years — started on medication because their TSH was elevated, now "stable" on replacement — who still feel awful.
When we look at their full thyroid panel, the picture often becomes clear: their TSH has been brought into range, but their free T3 — the active hormone their cells actually use — is at the very bottom of the reference range. Not below normal. Just not optimal. And because "TSH is normal" is the only metric that's been tracked, the insufficient conversion of T4 to T3 has never been identified or addressed.
Nobody asked the wrong question. Everyone asked "is the TSH normal?" and got "yes." But nobody asked "is the full thyroid picture optimal?" — and the answer to that question is where the clinical value actually lives.
A Month in Review: What We've Covered Together
This is the final episode of March, and I want to take a moment to draw the threads together — because the four topics we've covered this month are not four separate things. They're one picture, viewed from four angles.

“AND NEXT WEEK WE’VE GOT ELI BRECHER - HOST OF GUT360 PODCAST - JOINING ME.”
If you've been following along this month: thank you. The response to these episodes has been one of the things that reminds me why this work matters. The number of people I've heard from who said "this is the first time someone has explained why I feel the way I do" — that's the whole point of what I'm building with the podcast and with everything else.
April is going to go deeper into metabolic health specifically — fasting insulin, blood sugar variability, and the cardiometabolic picture that underlies so much of the fatigue and cognitive dysfunction I see. I think it's going to be one of those months where a lot of pieces click into place.
If March has resonated and you haven't started somewhere yet: the Reset is £7.99 and gives you a whole-system first week that addresses everything we've talked about this month at a practical level. That's where I'd start. Everything else builds from there.
Start somewhere.
If you've spent years being told everything is normal while knowing something is off — the Reset is where the practical work begins. One week, one framework, one coherent first step.